CASE REPORT
Surgical pelvic limb amputation and tarsorrhaphy in an American Toad (Bufo americanus)
Chloe R. Dupleix & Samantha J. Sander
Department of Veterinary Clinical Medicine, College of Veterinary Medicine, University of Illinois, Urbana-Champaign, IL, USA
Abstract
An adult male American toad (Bufo americanus) was presented to the Wildlife Medical Clinic at the University of Illinois by a member of the public after finding the toad trapped in a window well. On presentation, the toad was quiet, alert and responsive. There was an inflamed lesion at the level of the left tarsus with a section of calcaneum protruding from the wound. Initial stabilization was performed, followed by surgical amputation at the mid-tibiofibula of the left pelvic limb three days after initial presentation. The surgery was successful, and the toad recovered well from anaesthesia. Two days after the procedure, corneal edema was appreciated in the right eye consistent with acute bullous keratopathy. Initial medical management was unsuccessful, necessitating a right unilateral tarsorrhaphy. One month after initial presentation, the toad had healed from all procedures, was eating well and was manoeuvring around the enclosure appropriately. Permanent placement at a zoological facility was elected due to the extent of surgical intervention necessary for this case. This case highlights analgesic considerations, pelvic limb amputation and ophthalmological procedures that may be a plausible option for treating anurans in a wildlife setting.
Keywords: American toad; amputation; tarsorrhaphy; wildlife rehabilitation
Citation: Wildlife Rehabilitation Bulletin 2025, 43(1), 1–6, http://dx.doi.org/10.53607/wrb.v43.291
Copyright: Wildlife Rehabilitation Bulletin 2025. © 2025 C. Dupleix. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Accepted: 14 November 2024; Published: 1 August 2025
Correspondence: Chloe R. Dupleix, Wildlife Medical Clinic at the University of Illinois, 2100 S. Goodwin Ave., Urbana, IL 61802. Email: dupleix3@illinois.edu
Introduction
Reasons for wild animals to be presented for care in a wildlife rehabilitation setting are generally grouped into four main categories: infectious, traumatic, habitat loss or neonatal/orphaned (Miller et al. 2023). Anurans specifically present for care most often due to traumatic injuries, like crushing injuries to the limbs or pelvis (Stocker 2005). As toads migrate in early spring, they are frequently injured while crossing roads and highways, underscoring the impact of anthropogenically produced traumatic events to this group (Stocker 2005).
In cases where limb sparing efforts are not possible after trauma, limb amputation may be necessary (Stocker 2005; ACVS n.d.). In a wildlife rehabilitation framework, however, humane euthanasia is often pursued in place of amputation. Removal of anatomical structures typically renders the animal non-releasable due to the permanent impact such a procedure would have on a wild animal (Miller 2012). Amputation often impacts the ability of wildlife to successfully find food, make nests and carry out normal activity for the species (Miller 2020). In cases when amputation of a body part would not hinder an animal’s normal activity, and other efforts to salvage the affected region cannot be successful, removal of that part would be acceptable. In these cases, careful consideration must be made regarding the impacts of amputation. Consideration includes evaluating the animal’s physical readiness, life stage, release habitat and species natural history (Miller 2012). This is to predict if that case can reasonably be expected to adapt to the change and fully function in their natural environment upon release (Miller 2012; Meredith 2016).
This paper discusses an example of amputation performed for a wild animal with consideration for the long-term implications of this procedure. Analgesia considerations and two different problems, and the corresponding surgical techniques, are discussed in this paper.
Case report
In November 2021, a 43.5 g adult male American toad (Bufo americanus) was presented to the Wildlife Medical Clinic at the University of Illinois after a member of the public found the toad trapped in a window well. On presentation, the toad was quiet, alert and responsive and was noted to be in good body condition based on the symmetric and appropriate muscle mass of the limbs and the round appearance of the coelom. Physical examination, including evaluation of the eyes, ears, oral cavity, coelom, skin, forelimbs, right pelvic limb, cardiac system and mentation, was considered normal. The toad’s left pelvic limb had an open wound at the level of the tarsus encompassing approximately 33% of the limb circumference. Bone exposure of the calcaneum was also appreciated (Fig. 1a). Peripheral granulation tissue was appreciated around the wound, suggesting the lesion was not acute. A positive withdrawal reflex was elicited for the limb upon manipulation of the limb. During the examination, the toad exhibited motor function of the leg as he was using the limb to ambulate. However, the toad was minimally bearing weight on the affected limb, and a shortened stride was noted.
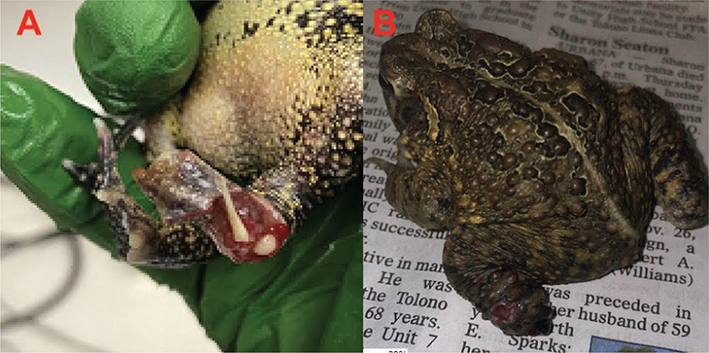
Figure 1 (a) Left leg of the American toad on presentation. The bones extruding from the surrounding tissue are the head of the tibiofibula and a section of the calcaneum. (b) Healed left hind limb five weeks post-amputation.
At initial presentation, the wound was gently and copiously lavaged with dilute chlorhexidine gluconate (VetOne®, MWI Veterinary Supply Co., Boise, ID), followed by warm lactated ringer’s solution (ICU Medical, Inc., Lake Forest, IL). A thin layer of 1% silver sulfadiazine cream (King Pharmaceuticals, Inc., Bristol, TN) was applied to the wound, and meloxicam (1.5 mg/ml, Meloxidyl, VetOne®, MWI Veterinary Supply Co., Boise, ID, 0.4 mg/kg) was administered by mouth. Supportive care and wound care, including daily application of silver sulfadiazine cream and meloxicam, were performed for three days until additional diagnostics and interventions could be pursued.
Three days after presentation, this toad was sedated for survey radiographs and a partial left pelvic limb amputation surgery. The toad was anaesthetized in a shallow bath of 1 g/L buffered tricaine methanesulfonate (MS-222; Syncaine®, Syndel Laboratories Ltd., Ferndale, WA). To facilitate safe induction, non-woven gauze squares were placed under the toad to ensure the toad’s head was maintained above the waterline. A working depth of anaesthesia was achieved once gular respirations slowed, palpebral reflexes were absent and no muscle tone or withdrawal reflex was appreciated. Both eyes were lubricated with artificial tears (Soothe Lubricant Eye Ointment, Bausch + Lomb, Rochester, NY) while anaesthetized. Patient monitoring during this event included the use of Doppler ultrasound for heart rate and visual assessment of gular movement for respiration rate.
Radiographs of the toad positioned in a frog-legged dorsoventral view and an extended-legged dorsoventral view were obtained (Fig. 2a, b). Orthogonal views were not obtained due to technical error. Radiographic evidence of osteomyelitis was not appreciated in the left calcaneum, tibiofibula or femur. Most of the metatarsal bones and digits on the affected limb were missing, as they had sloughed despite gentle handling during the radiographic procedure.
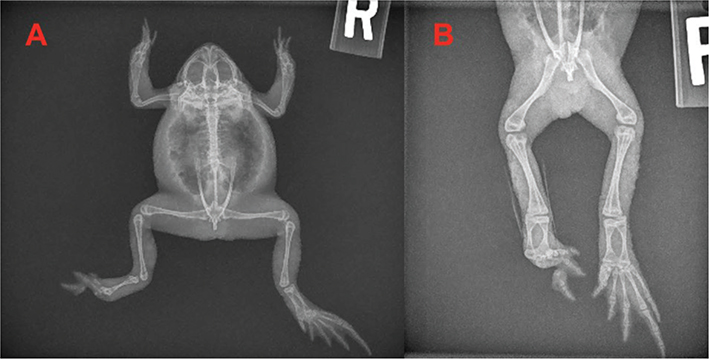
Figure 2 (a) Pre-surgical radiograph of the American toad in a frog-legged dorsoventral view. (b) Pre-surgical radiograph of the American toad in an extended-legged dorsoventral view.
Complete limb sparing efforts were not considered possible given the extent of the injury. Indicators such as auto-amputation near the distal lesion, partial skin necrosis at the affected site and the presence of chronic bone exposure suggested the limitations of this approach. Considering the toad’s functional use of the limb and the absence of evident pathology proximal to the lesion, the decision was made to perform a partial limb amputation at the site of the lesion. This choice aimed to preserve the remaining limb function and eliminate the persistent site of disease and perceived pain in this case.
Surgical amputation was pursued in the same anaesthetic event in which the radiographic assessment had occurred. The toad was placed in sternal recumbency on a stack of non-woven gauze squares soaked in 1 g/L MS-222. The limb was prepped, and a tourniquet made from sterile central IV-line tubing was placed around the left proximal leg and secured with haemostats. Using sterile surgical technique, the skin and soft tissue around the tibiofibula were bluntly dissected from the tibiotarsal joint using tissue scissors and Adson Brown forceps until the joint was adequately exposed. A #11 surgical blade was used make a complete mid-diaphyseal transection of the mid-tibiotarsus. The remaining soft tissue was closed around the proximal tibiotarsus using 4-0 poliglecaprone 25 suture (MONOCRYL™ (poliglecaprone 25) Suture, ETHICON©, Ethicon US, LLC, Raritan, NJ) in a two-layer simple interrupted pattern. Throughout this procedure, heart rate was monitored via Doppler ultrasound, and gular movements were monitored as an indication of spontaneous respiration.
Upon surgical completion, the toad was placed in sternal recumbency on a disposable underpad soaked in LRS over a heating pad for anaesthetic recovery. An injection of ceftazidime (10 mg/ml, Tazidime®, Eli Lilly and Company, Indianapolis, IN, 20 mg/kg) was administered intramuscularly in the left thoracic limb. Recovery was smooth, quick and uneventful. When the toad was fully recovered, meloxicam (0.4 mg/kg, 1.5 mg/ml) was administered by mouth. Post-operative management included empiric antibiotic therapy with ceftazidime (20 mg/kg, 10 mg/ml) injected intramuscularly every three days for six doses, and analgesia with meloxicam (0.4 mg/kg, 1.5 mg/ml) by mouth once per day for 25 doses. Daily assessment of surgical site healing and maintaining the animal in a clean, moist environment were also pursued. Three-month post-operative radiographs were obtained and showed no evidence of infection or other abnormalities associated with the left pelvic limb (Fig. 3).
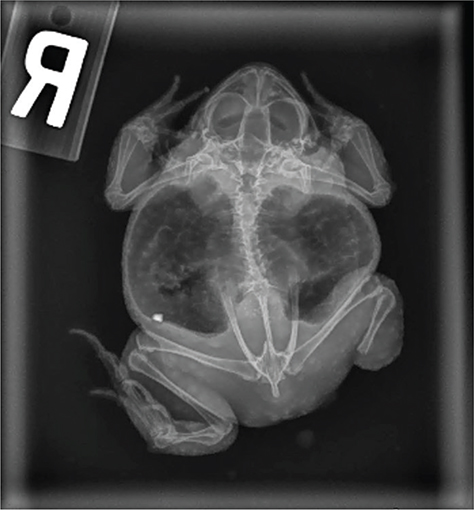
Figure 3 Three-month post-operative radiograph of the American toad in a relaxed, unpositioned dorsoventral view. No evidence of disease is appreciated in the affected limb in either the skeleton or soft tissue.
The toad’s right eye appeared edematous and cloudy the day following the amputation procedure. Empiric treatment was initiated with one drop of hypertonic ophthalmic 5% sodium chloride solution (Major® Pharmaceuticals Rugby® Laboratories, Livonia, MI) applied topically in the right eye twice per day. After two days using this medication, mucopurulent discharge was appreciated from the right eye. Administration of one drop of ofloxacin 0.3% ophthalmic solution (Bausch + Lomb Inc., Bridgewater, NJ) topically to the right eye twice per day was added to the treatment protocol. The antibiotic was administered first, and then hypertonic saline was administered after five minutes of contact time. The toad received both medications for a total of 13 days prior to consulting with the Ophthalmology Service at the University of Illinois. During this consultation, a fluorescein stain of the right eye and examination with a slit lamp led to a diagnosis of acute bullous keratopathy (Fig. 4a). Based on the timeline of clinical signs, the bullous keratopathy may have been caused by accidental exposure of MS-222 to the right eye during the toad’s anaesthetized amputation procedure. A modified temporary tarsorrhaphy procedure was elected after a poor response was seen with the medical management alone.
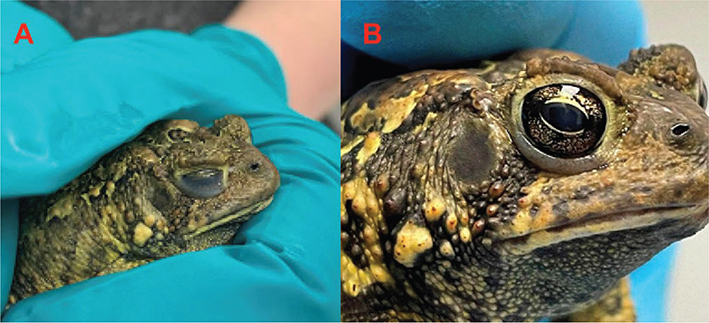
Figure 4 (a) Bullous keratopathy of the right eye. (b) Healthy right eye two weeks after the temporary tarsorrhaphy was placed.
A 1 g/L MS-222 dilution containing 102 g of dechlorinated water, 0.1 g of MS-222 and 0.14 g of sodium bicarbonate was prepared in efforts to ensure the pH was as close to neutral as possible. However, the pH of the water was not quantified prior to the procedure due to the technical error. The toad was placed on buffered MS-222 gauze squares to facilitate transcutaneous absorption of the anaesthetic. Heart rate was monitored via Doppler ultrasound, and respirations were monitored via gular movement. When the toad was adequately anaesthetized to a working depth, one drop of cyanoacrylate glue was used to adhere the false nictating membrane to the superior eyelid, and the eyelid was held in place until dry. The patient recovered successfully and quickly in a warm dechlorinated water bath. While the tarsorrhaphy was in place, the topical eye medications were temporarily discontinued.
The right eye spontaneously opened five days after the ocular procedure, at which time topical hypertonic ophthalmic 5% sodium chloride solution was restarted. Upon re-examining the toad’s right eye, corneal edema was still present with markedly reduced severity. Treatment was continued daily for four additional weeks; at which time, all gross evidence of the bullous keratopathy had resolved (Fig. 4b).
Meloxicam was discontinued for the toad four weeks after initial presentation, based on clinical resolution of inflammatory signs at the leg amputation site. At this time, the amputation site was considered healed (Fig. 1b). The toad remained in care for several months for monitoring and supportive care, as it was seasonally inappropriate to consider this animal for release at the time of healing. Throughout that time, this toad was able to eat on his own, he exhibited appropriate locomotion and behavioural responses to his environment and he generally appeared to be in good health. Based on these behaviours, this toad was considered a potential candidate for release. The outcome for the toad was permanent placement in an accredited zoological facility, as some concerns persisted about its ability to fully function in the wild with a partial hind limb amputation.
Summary
Amputation of limbs or other modification of body parts requiring extensive change in natural husbandry is not commonly recommended in the field of wildlife rehabilitation medicine (Miller 2012). This thought process is maintained by several wildlife rehabilitation medical facilities, including the Wildlife Medical Clinic at the University of Illinois. In the case of this American toad, the location of the lower leg amputation was not observed to overtly permanently disable or compromise the welfare and survival of this animal in the wild. If compromise was observed, this animal would have met criteria for euthanasia of wild animals with traumatic amputation lesions (Meredith 2016).
There are documented instances of injured wild animals returning to the wild post-amputation. In some wildlife veterinary practices, owls with unilateral traumatic ocular injuries will undergo eviscerations of the affected eye prior to release (Murray et al. 2013). Owls retain the ability to hunt with one eye based on their unique ocular and head anatomy, making them a good potential candidate for this type of procedure. It should be noted that not all uniocular owls can adapt to facilitate appropriate welfare and survival in the wild, however (Murray et al. 2013). Additionally, multiple species of sea turtles have been released post-flipper amputation and have been documented to ambulate similarly to those with all four limbs intact (Robinson et al. 2021). Observing appropriate ambulation was imperative for the toad prior to release, thus supporting the likelihood this animal could be successful in the wild upon potential release.
Toads, like other anurans, use their hindlimb muscles as the primary producers of power for jumping and ambulation (Gillis et al. 2014). These muscles include four large muscle bodies (Gillis 2007). The iliacus externus muscle originates from the ilium and inserts onto the head of the femur for aiding in hip flexion, while the iliofibularis muscle runs along the dorsal aspect of the thigh and inserts onto the proximal tibiofibula to allow the knee to flex (Gillis 2007). The semitendinosus muscle has two heads, which originate off the pelvic rim and converge to form one tendon (Gillis 2007). This tendon inserts onto the proximal tibiofibula also for flexion of the knee (Gillis 2007). Finally, the tibialis anticus longus originates on the proximal tibiofibula and inserts onto the os fibulae and os tibiale to flex the ankle joint (Gillis 2007). All muscles and the tendonous attachment described for anuran ambulation were left fully, if not mostly, intact in this American toad.
Landing after take-off is just as important when evaluating the kinetics of anuran ambulation (Gillis et al. 2014). Toads use substantial amounts of their forelimbs and pectoral girdle movements to land successfully (Griep et al. 2013). American toads have been documented to flex their hindlimbs mid-jump to prepare for the landing sequence (Gillis et al. 2014). The American toad in this case was observed extensively for the appropriate leg movements allowing full hops. This was seen as the toad would hunt for the provided prey item in his hospitalization enclosure.
Besides ambulation, evaluating the function of a toad’s eye is crucial for his survival (Levine et al. 2004). Many anuran species retract their eyes repeatedly during swallowing as this motion aids to push food towards the oesophagus (Levine et al. 2004). Before and after performing the temporary tarsorrhaphy, ensuring this function remained intact was essential for the success of this toad in the wild. This animal was observed hunting prey and increased 22% in body weight throughout his hospitalization, suggesting this animal retained function in both eyes to support hunting and swallowing of prey.
In this case report, the toad developed an acute bullous keratopathy after a prolonged anaesthetic event with a buffered MS-222 bath. Bullous keratopathy is characterized by blister-like swelling of the cornea that can lead to bright light sensitivity, blurred vision and intermittent irritation (Roat 2022). MS-222 has a low pH if not diluted properly and can cause severe irritation and damage to delicate tissues, like in the eye. Bullous keratopathy in wildlife has been reported in avian species, with an excellent prognosis depending on the mode of treatment (Barbon & Kubiak 2020). Most often, bullous keratopathies are treated by temporary tarsorrhaphy of the affected eye (Irving et al. 2023). This form of treatment was successful for the case of this American toad.
All treatments and procedures provided for this case were effective in optimizing this animal for release. The criteria put in place for this toad to be released included the ability to effectively ambulate post-amputation, the ability to hunt and eat prey items in the enclosure, and demonstration of normal anuran activity such as soaking, hiding and interacting with objects in his environment. Each criterion was met. Despite this, permanent placement was elected out of caution due to persistent concerns about potential long-term impacts on ambulation, given the partial leg amputation procedure.
This case illustrates an example of effective analgesia and antibiotic usage in anurans, the possibility to perform distal limb amputation for wild toads and a modified temporary tarsorrhaphy as an effective treatment method of bullous keratopathy in an anuran species.
Acknowledgements
The authors would like to thank Billy Wright for his contributions to the management of this case and manuscript.
References
| ACVS.org [homepage on the Internet]. n.d. Limb Amputation. Accessed on the internet at https://www.acvs.org/small-animal/limb-amputation/ on 13 January 2024. |
| Barbon A.R. & Kubiak M. 2020. Birds of prey. In M. Kubiak (ed.): Handbook of exotic pet medicine. Pp. 189–218. First edition. Hoboken, NJ: Wiley-Blackwell. |
| Gillis G.B. 2007. The role of hind limb flexor muscles during swimming in the toad, Bufo marinus. Zoology 110, 28–40, doi: 10.1016/j.zool.2006.08.002 |
| Gillis G., Ekstrom L. & Azizi E. 2014. Biomechanics and control of landing in toads. Integrative and Comparative Biology 54(6), 1136–1147, doi: 10.1093/icb/icu053 |
| Griep S., Schilling N., Marshall P. & Amling M. 2013. Pectoral girdle movements and the role of the glenohumeral joint during landing in the toad, Rhinella marina (Linnaeus, 1758). Zoomorphology 132(3), 325–338, doi: 10.1007/s00435-013-0189-0 |
| Irving W., Whittaker C., Caruso K., Reynolds B., McCarthy P. & Smith J. 2023. Bullous keratopathy in a dwarf rabbit (Oryctolagus cuniculus domesticus). Journal of Exotic Pet Medicine 47, 23–26, doi: 10.1053/j.jepm.2023.07.003 |
| Levine R.P., Monroy J.A. & Brainerd E.L. 2004. Contribution of eye retraction to swallowing performance in the northern leopard frog, Rana pipiens. Journal of Experimental Biology 207, 1361–1368, doi: 10.1242/jeb.00885 |
| Meredith A. 2016. Wildlife triage and decision-making. In E. Mullineaux & E. Keeble (eds.): BSAVA manual of wildlife casualties. Pp. 27–36. Second edition. Quedgeley, England: Waterwells Business Park. |
| Miller E.A. 2012. Final disposition. In E.A. Miller (ed.): Minimum standards for wildlife rehabilitation. Pp. 74–80. Fourth edition. St. Cloud, MN: National Wildlife Rehabilitators Association. |
| Miller E.A. 2020. Natural history and management of squirrels and other rodents. in S.M. Hernandez, H.W. Barron, E.A. Miller, R.F. Aguilar & M.J. Yabsley (eds): Medical management of wildlife species: A guide for practitioners. Pp. 169–184. First edition. Hoboken, NJ: Wiley-Blackwell. |
| Miller T.K., Pierce K., Clark E.E. & Primack R.B. 2023. Wildlife rehabilitation records reveal impacts of anthropogenic activities on wildlife health. Conservation Biology 286, 110295, doi: 10.1016/j.biocon.2023.110295 |
| Murray M., Pizzirani S. & Tseng F. 2013. A technique for evisceration as an alternative to enucleation in birds of prey: 19 cases. Journal of Avian Medicine and Surgery 27(2), 120–127, doi: 10.1647/2012-007 |
| Roat M.I. 2022. Bullous keratopathy. Accessed on the internet at https://www.merckmanuals.com/professional/eye-disorders/corneal-disorders/bullous-keratopathy on 9 October 2023. |
| Robinson D.P., Hyland K., Vettan A., Mabadikate A., Jabado R.W., Rohner C.A., Pierce S.J. & Baverstock W. 2021. Satellite tracking of rehabilitated sea turtles suggests a high rate of short-term survival following release. PLoS One 16(2), e024624, doi: 10.1371/journal.pone.0246241 |
| Stocker L. 2005. Fracture management. In L. Stocker (ed.): Practical wildlife care. Pp. 67–87. Second edition. Ames, IA: Blackwell Publishing. |